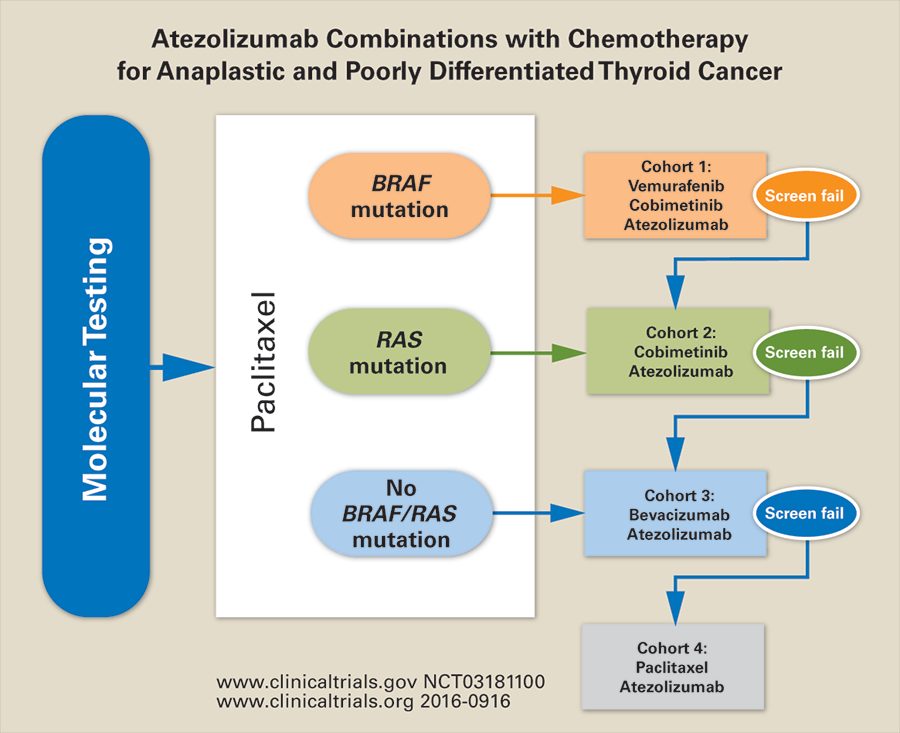
试验结合atezolizumab目标或cytotoxic agents for patients with anaplastic or poorly differentiated thyroid cancer
September 2017 : Laser Interstitial Thermal Therapy for Spinal Metastases
Laser Interstitial Thermal Therapy for Spinal Metastases
Laser technique may be alternative to open surgery prior to stereotactic radiation therapy for metastases adjacent to the spinal cord
Magnetic resonance imaging shows epidural spinal metastases (arrows) before (left) and after (right) treatment with spinal laser interstitial thermal therapy. Images courtesy of Dr. Claudio Tatsui.
In many patients with spinal metastases, stereotactic radiation therapy can provide effective local tumor control to prevent spinal cord compression and subsequent paralysis. However, in patients in whom a metastasis is touching or displacing the spinal cord, the tumor must be separated from the spinal cord before stereotactic radiation can be safely delivered. Until recently, this meant that such patients would have to endure an open surgery, along with its attendant potential complications and delays in other oncological treatment. But now a surgeon at The University of Texas MD Anderson Cancer Center is adapting an existing ablation method as an alternative to surgery to treat spinal metastases in select patients.
To avoid the risks associated with surgery for spinal metastases, Claudio Tatsui, M.D., an associate professor in the Department of Neurosurgery, has adapted a laser-based thermal ablative technique routinely used to treat tumors in the brain, prostate, liver, and other sites. The resulting procedure, spinal laser interstitial thermal therapy (SLITT), is currently performed only at MD Anderson.
Instead of having to surgically remove the portion of the tumor adjacent to the dura mater prior to stereotactic radiation therapy, Dr. Tatsui said, “We’re using a laser to heat and destroy the tumor in the epidural space and then covering the residual disease with stereotactic radiation therapy.”
Performing the procedure
In SLITT, a Jamshidi bone marrow needle is advanced into the spinal metastasis under magnetic resonance imaging (MRI)– or computed tomography–based guidance. The needle’s central trocar is removed, and a Kirschner wire is inserted through the needle. The Jamshidi needle is then removed, leaving the Kirschner wire to serve as a guide for placing an access cannula. Additional cannulas are usually placed; the number used depends on the size and location of the tumor.
For the ablation step, a laser probe is advanced to the end of the access cannula in the tumor, and the cannula is retracted slightly to expose the tip of the laser probe. The probe is then energized to heat the surrounding tissue to a temperature that irreversibly damages tumor cells (typically 50–74°C); the temperature at the interface between the tumor and vital structures is maintained at less than 50°C to avoid damaging those structures. The heating process is monitored in real time with MRI thermometry.
“What makes this procedure special is not the temperature itself, but the monitoring of the temperature in space,” Dr. Tatsui said. “The MRI lets me localize the temperature and treat lesions near vital organs without damaging those structures. We can find in real time where the heat is being applied, the extent of the damage, and if there is a need for additional laser probes.”
The heating process is repeated several times to ensure adequate thermal coverage of the tumor. The laser probe can deliver tumor-killing temperatures within a radius of 5–7 mm; and typically three access cannulas are needed per spinal lesion, although Dr. Tatsui said that he has used as many as eight cannulas for very large tumors. Preparing each cannula takes about 1 hour, but the ablation procedure itself takes only 3 or 4 minutes, depending on the complexity of the case. The procedure can be repeated as many times as needed if the tumor grows back.
As with traditional open surgery, SLITT is followed by stereotactic radiation therapy. But SLITT enables a much quicker return to treatment than does surgery. Whereas the median hospital stay following surgery is 7 days, that following SLITT is only 2 days, Dr. Tatsui said, noting that the procedure can also benefit patients for whom a long interruption in systemic treatment is not ideal.

During spinal laser interstitial thermal therapy, magnetic resonance imaging thermometry shows the real-time temperature at the preset monitoring point and safety stops (orange and green boxes, respectively, in degrees Celsius) around the laser probe, allowing the surgeon to ensure that the laser heats the tumor tissue, but not nearby vital structures, to a temperature that causes irreversible damage. (The red and yellow area is a heat artifact caused by the patient’s heartbeat, not the laser.) Image courtesy of Dr. Claudio Tatsui.
Another benefit of SLITT is that it appears to be substantially less painful than open surgery. “We’ve looked at patients’ self-reported pain scores before and after the procedure, and we haven’t seen the immediate increase in pain that we see with standard open surgery,” Dr. Tatsui said.
Selecting the right patients
Dr. Tatsui has used SLITT followed by stereotactic radiation to treat epidural spinal metastases from melanoma and from breast, lung, prostate, and other cancers but has most often used it in patients with metastases from renal cell carcinoma, which is notoriously resistant to chemotherapy and conventionally fractionated radiation therapy. “We’re using this technique to treat pretty much any metastatic tumor in the epidural space that is resistant to conventional radiation therapy,” he said.
The procedure has the most benefit in patients with metastatic tumors in the thoracic spine, where about 70% of spinal metastases occur. Dr. Tatsui said he tries to avoid performing SLITT in patients with metastases in the lumbar spine because these tumors can involve or abut motor nerves, which are very sensitive to heat.
“I’ve had two cases where the tumor was near a motor nerve and the patients had dysfunction of the nerve after SLITT,” Dr. Tatsui said. “So we tend to do the procedure where there are only sensory nerves. The thoracic spine, from T2 to T12, is where we get the best results with this technique.”
SLITT has also been used without stereotactic radiation in eight patients, Dr. Tatsui said. These patients had already received the maximum cumulative dose of radiation to the spine and were not strong candidates for palliative surgery because of the scarring from radiation and the associated poor healing. The results were promising, Dr. Tatsui said, and if the tumors recur, SLITT can be repeated.
Although SLITT could be used to treat primary tumors in the spine, Dr. Tatsui said, such tumors are probably more effectively treated with appropriate oncological (i.e., radical) resection.
Looking forward
Dr. Tatsui said that he and his colleagues have been very pleased with what they’ve observed in combining SLITT with stereotactic radiation therapy, and a pilot study (No. 2015-0481) evaluating the safety and accuracy of intraoperative MRI guidance for SLITT is ongoing. Now, he said, “We’re retrospectively comparing outcomes of our laser ablation protocol with those of open surgery, and we’re observing very positive results. We plan a future prospective study to directly compare SLITT and open surgery in the management of spinal metastasis.
“I envision that this will be an alternative to open surgery, especially for patients with aggressive systemic disease or significant comorbidities that preclude surgery,” Dr. Tatsui said.
For more information, contact Dr. Claudio Tatsui at 713-563-8710 orcetatsui@mdanderson.org.
FURTHER READING
Tatsui CE, Stafford J, Li J, et al. Utilization of laser interstitial thermotherapy guided by real-time thermal MRI as an alternative to separation surgery in the management of spinal metastasis. J Neurosurg Spine. 2015;23:400–411.
OncoLog62年,2017年9月,体积问题9
More Stories From OncoLog
A New Era in Follicular Lymphoma
Newly approved drugs, clinical trials represent shift from cytotoxic to targeted and immunotherapeutic agents

House Call: Understanding Clinical Trials
Trials provide access to new cancer treatments
